Hospital readmissions cost Medicare alone more than $24 billion in 2011 (Hines et al., 2014). Legislation embedded in the Patient Protection and Affordable Care Act aimed at reducing readmissions levies penalties against hospitals with higher than average readmission rates. These penalties were expected to increase to $566 million in 2019 (Allen, 2019). Bridging the Discharge Gap Effectively (BRIDGE) is a nurse practitioner-led, transitional care cardiology clinic designed to reduce unnecessary hospitalizations.
Hospital readmissions cost Medicare alone more than $24 billion in 2011 (Hines et al., 2014). Legislation embedded in the Patient Protection and Affordable Care Act aimed at reducing readmissions levies penalties against hospitals with higher than average readmission rates. These penalties were expected to increase to $566 million in 2019 (Allen, 2019). Bridging the Discharge Gap Effectively (BRIDGE) is a nurse practitioner-led, transitional care cardiology clinic designed to reduce unnecessary hospitalizations.
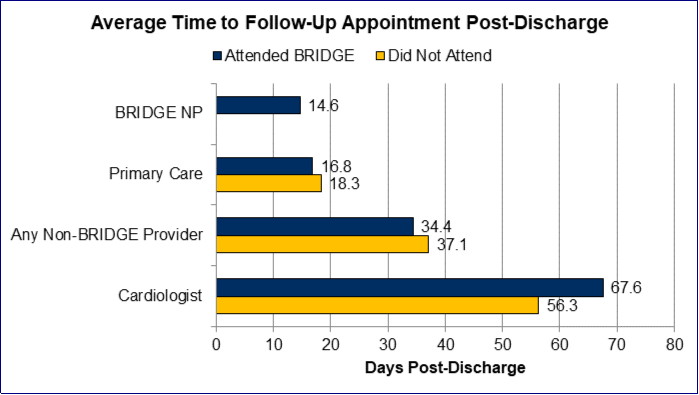
BRIDGE strives to facilitate patients’ transition from hospital to home by serving as an extension of the in-patient care team. The clinic aims to schedule patients within fourteen days of hospital discharge. At these 60 minute visits, nurse practitioners assess each patient’s status and response to treatment, educate patients on cardiovascular disease and lifestyle modifications, and make evidence-based medication and therapy adjustments when necessary (Bumpus et al., 2017).
Through our research at MCORRP, we have found that most patients presenting to the clinic were referred due to acute coronary syndrome (ACS), congestive heart failure (CHF), or atrial fibrillation (AF). In a recent study of over 2400 cardiac patients, acute coronary syndrome patients who attended BRIDGE were significantly less likely to be readmitted within 30 days than those who did not attend (6.4% vs. 13.1%, p=0.006) (Bumpus et al., 2017). Further, over the course of one year, BRIDGE demonstrated a significant cost savings for ACS patients as a result of avoided rehospitalizations within 30 days of index discharge. On average, the utilization of this intervention translated into a $4,944 per-patient savings. Stated another way, BRIDGE saved $306,537 in annual healthcare costs at our health system for ACS patients alone. Not only were patients less likely to be readmitted if they attended, they were also less costly to manage (Bumpus et al., 2016).
The BRIDGE database is continually being updated to provide a more robust sample for measuring the outcomes of this program. Six BRIDGE-related abstracts were accepted for presentation at national conferences in 2020. These abstracts, developed by students, explored the following: 1) substance use among patients referred to BRIDGE 2) characteristics of heart failure patients by time to readmission 3) characteristics of acute coronary syndrome patients by time to readmission, 4) inpatient sleep interruptions among congestive heart failure patients, 5) outcomes of patients with depression with and without antidepressant prescription, and 6) the effectiveness of the BRIDGE transitional care clinic. Additionally, two manuscripts, which examined 1) readmission patterns of atrial fibrillation patients, and 2) the relationship between patient satisfaction and outcomes, were published in peer-reviewed journals.